Article Text

Statistics from Altmetric.com
- long-acting reversible contraception
- intrauterine devices
- Contraceptive Devices, Female
- Reproductive Health Services
- contraception behavior
Many women in the UK find it difficult to access the contraceptive services they need.1 Long-acting reversible contraception (LARC) has been highlighted as a key area for improvement, with the recommendation to introduce evidence-based technologies as a way of improving accessibility.2 In 2022/2023, LARC comprised 55% of contraception appointments at Integrated Sexual Health Services. Of these, the copper intrauterine device (Cu-IUD) and levonorgestrel intrauterine device (LNG-IUD) comprised 10% and 16%, respectively.3
Locala Community Partnerships CIC run three Integrated Sexual Health Services across the North of England. Prior to June 2023, patients requesting intrauterine contraception (IUC) would have a pre-procedure telephone consultation to assess eligibility and discuss the method and procedure. Clinician feedback noted high rates of repeated counselling at subsequent IUC fitting appointments. An alternative process was suggested and a standard operating procedure (SOP) designed. When patients contacted the service they were offered two booking options: either a telephone appointment following our original process, deemed ‘pre-counselling’, or alternatively they could forgo a telephone consultation and book into an IUC fitting appointment at initial service contact with a specifically designed information leaflet sent via SMS to read beforehand, deemed ‘direct booking’. We conducted a retrospective review of the quality improvement project to assess the impact of direct booking. It was thought that the introduction of direct booking would lead to less duplication of work, create efficiencies and improve accessibility. To ensure the process was acceptable to patients and staff we collected feedback throughout to highlight any unanticipated effects of the new system.
Records were reviewed over a 2-month period and data collected on booking method, eligibility for IUC fitting at appointment and indication for IUC (figure 1). Eligibility criteria applied at IUC fitting appointments followed Faculty of Sexual and Reproductive Healthcare (FSRH) and United Kingdom Medical Eligibility Criteria (UKMEC) guidelines.4 5

Diagram detailing data collection and analysis. Cu-IUD, copper intrauterine device; IUC, intrauterine contraception.
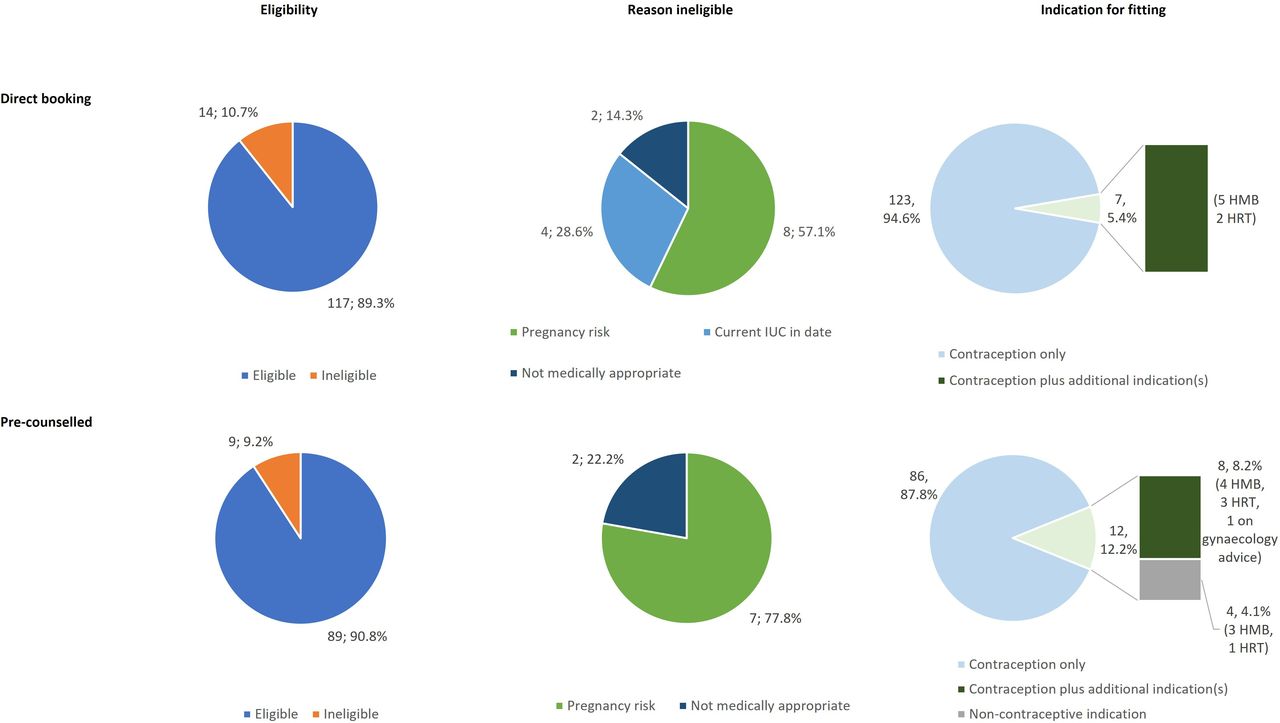
Our results showed there was very little difference in IUC eligibility between the two groups and that direct booking did not lead to increased insertions for non-contraceptive purposes, which would fall outside of our local commissioning.
Of those ineligible for fitting, 28.6% (4/14) of patients in the direct booking group were ineligible as their current IUC was not due for renewal compared with zero in the pre-counselled group (figure 2). On reviewing our pre-insertion leaflet we found there was no updated advice on extended use of IUC as per the FSRH 2023 guideline,4 which could be a reason for the small difference between the two groups. We amended the leaflet to reflect this and added a flow chart to explain pre-IUC pregnancy exclusion criteria.

{kind=link}
{kind=link}
Pie charts showing intrauterine contraception (IUC) eligibility, reason ineligible for IUC fitting, and indication for IUC in both direct booking and pre-counselled groups. HMB, heavy menstrual bleeding; HRT, hormone replacement therapy; IUC, intrauterine contraception.
A feedback survey was sent to all direct booking patients. Of 24 respondents, 22 agreed or strongly agreed that they were happy to be directly booked for IUC fitting and two strongly disagreed. Additionally, 23/24 agreed or strongly agreed that they had sufficient time at the fitting appointment for discussion and one patient strongly disagreed.
“Direct booking is most definitely the way forward. I was very happy with how quick my appointment was and the information I received about the procedure beforehand. Staff were very helpful and friendly throughout.”
“Simple and quick service.”
A pre-counselling telephone appointment is allocated 20 minutes; over the 2-month period, 132 patients opted for direct booking, saving 2640 min of clinician time. The length of time for fitting appointments remained the same for both booking methods. We continue to offer booking via either method.
We feel that by offering different options for IUC counselling there is greater accessibility for patients, potentially reducing barriers to LARC fitting. By involving patients and staff via regular feedback, areas for improvement can be identified quickly and implemented, with the SOP updated as time progresses. There were large efficiency gains to the service and feedback showed that direct booking was well perceived by patients and staff.
Ethics statements
Patient consent for publication
Footnotes
Contributors KF collected and analysed data, and wrote up the work for submission. MC suggested the project, developed the standing operating procedure, delivered staff training, and critically reviewed the written piece of work. RS critically reviewed the written piece of work and supported the project.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.